- HPI: 60s M woke up from sleep with chest pain radiating to the back with nausea x 1 hr
- Cath: 100% in-stent thrombosis of his prior RCA stent
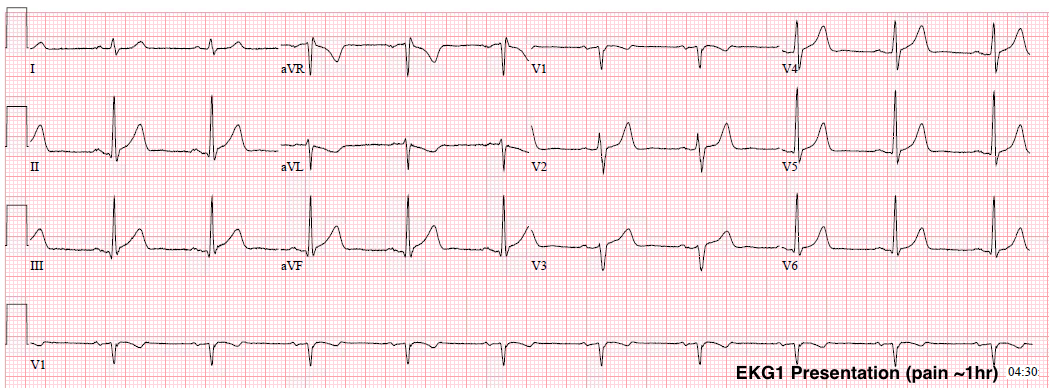
- Key ECG: No pathologic Q-waves. Without the prior ECG for comaparison, the T-waves are not clearly hyperacute. There is slight STE in V3-V5. There is 1-2mm STE in II, III, and aVF with slight J-point depression in aVL and marked, large T-wave inversion in aVL. If you consider only the ST elevation in the inferior leads out of context, this amount and morphology would not be incompatible with a baseline ECG of a young man with high voltage and diffuse baseline ST elevation. The ST depression and T-wave inversion in aVL, however, is NOT compatible with a baseline abnormality, and makes the ECG highly suspicious for acute coronary occlusion. As has been shown through many prior cases and publications by Dr. Smith, lead aVL holds the key to understanding inferior ST elevation. ST depression in aVL should always be assumed to be due to inferior MI, unless there is: limb lead LVH, WPW, LBBB, paced rhythm, etc. If there are well-formed Q-waves, it could be due to inferior LV aneurysm as well.
- Link to full case @ Dr. Smith’s ECG Blog: 2017-10-31