- HPI:50M with 24 hr worsening L-sided chest pain
- Cath: 3VD with 99% distal RCA (culprit) for which CABG was arranged
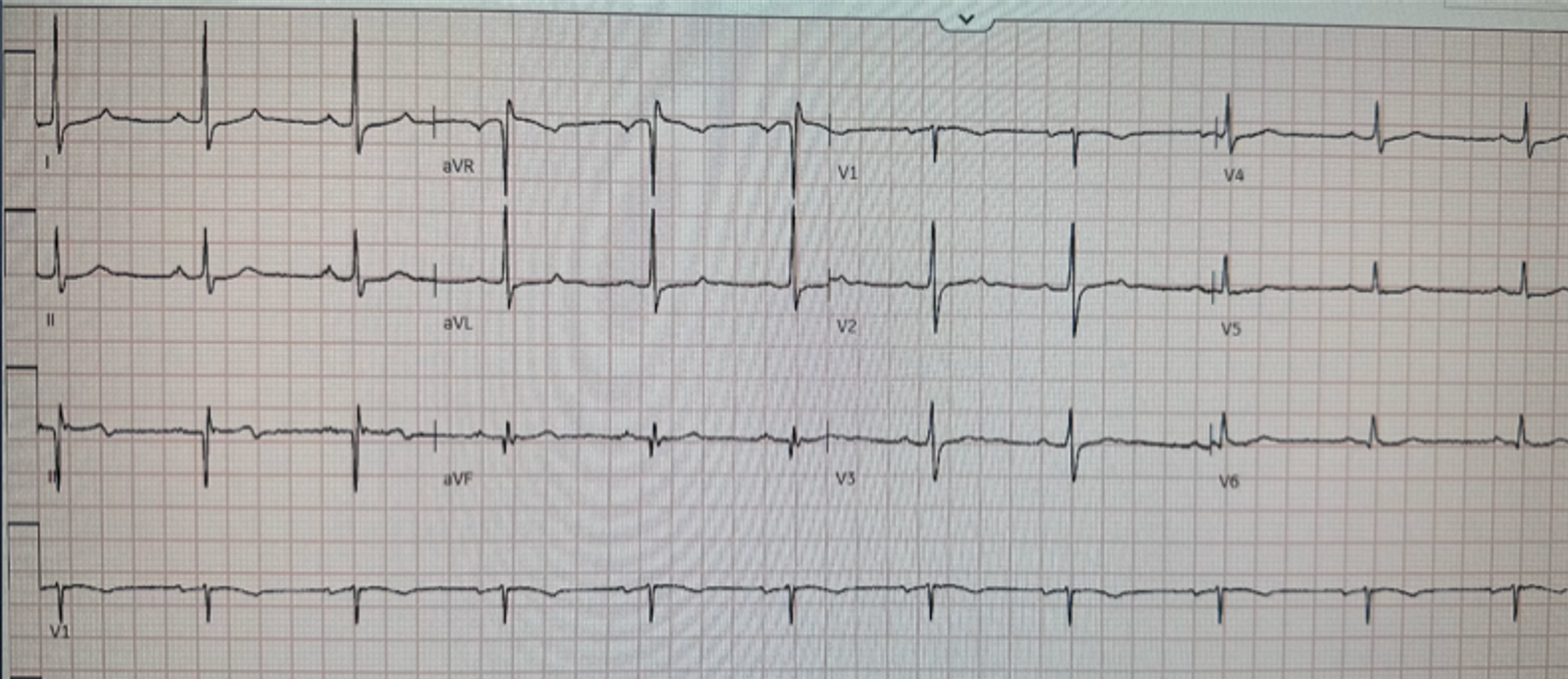
- Key ECG: Minimal STE in III, some STD in I and aVL, and terminal T wave inversion in III, suggesting some reperfusion. This is not specific for OMI, however if the patient has resolving chest pain this could be consistent with recent OMI, now with reperfusion ST-T. ECG findings suggests that *at some point in time* — the patient has had an inferior infarction: The Q wave in lead III is huge. There is also a significant Q wave in lead aVF — that is equal in depth to the height of the tiny R wave in this lead. These findings could represent multi-vessel disease, on top of which there may (or may not be) ECG changes of another new event.
- Link to full case @ Dr. Smith’s ECG Blog: 2023-04-09