- HPI: young adult with acute chest pain
- Cath: A 100% acute occlusion of the proximal LAD was found, and stented
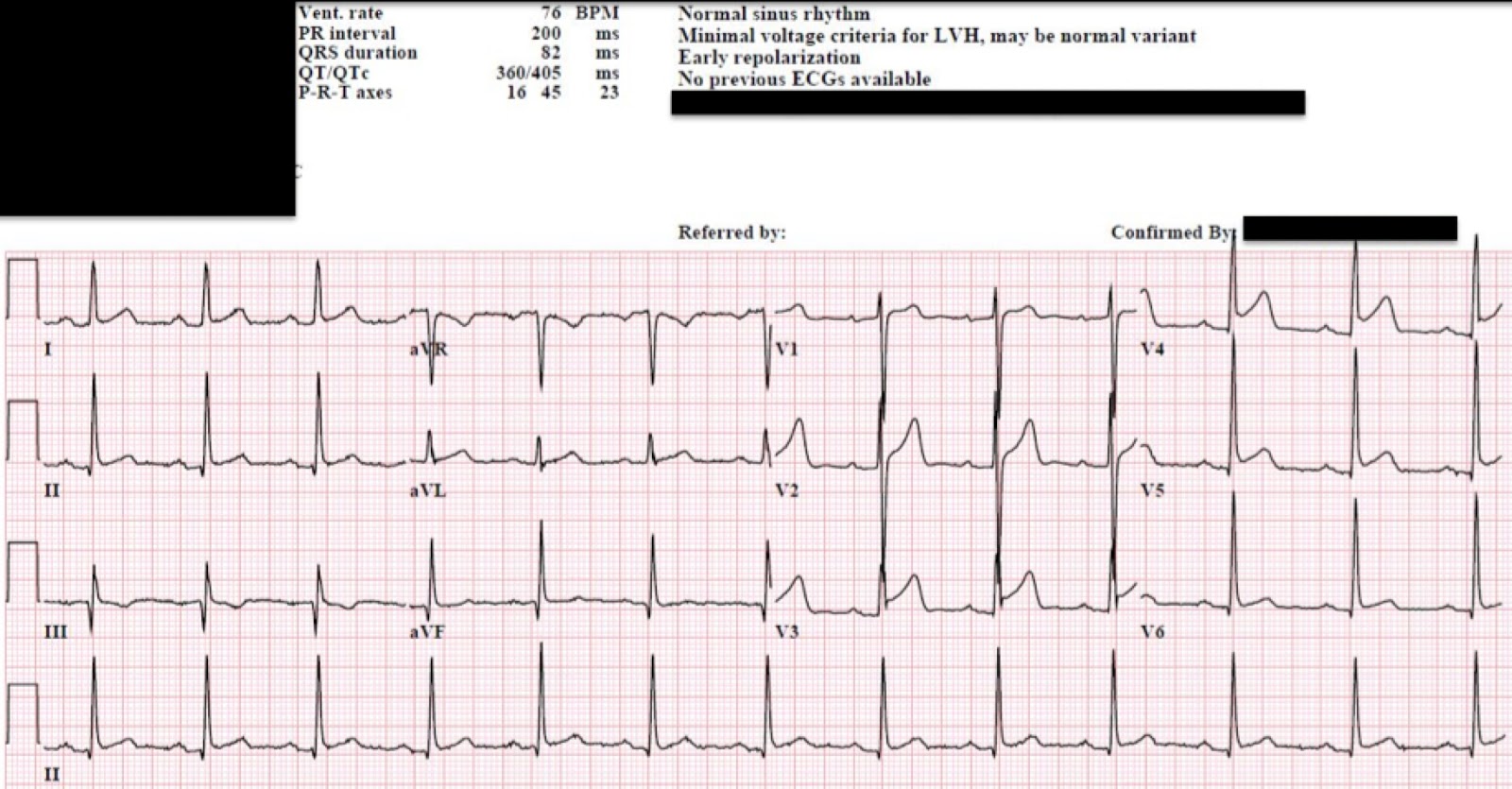
- Key ECG: There is ST segment elevation in multiple leads, most of which have an associated J-wave (slurring of the J-point); e.g. in V4-V6, I, II, and aVF. There is no reciprocal depression, the QTc is not significantly lengthened, and the ST segments in V2 – V4, although elevated, are concave upwards. All of these elements point to benign early repolarization. If you used the LAD occlusion vs. Early Repol formula you get 21.9 (which effectively excludes LAD occlusion). But you should not have used the formula for this case. Why not? Look at V3: There is no S-wave in this lead, and neither is there a J-wave. This loss of the S-wave is called terminal QRS distortion, and multiple studies suggest that, with an anterior MI, this predicts a larger infarct, with higher mortality, and even a worse response to fibrinolytics or PCI.
- Link to full case @ Dr. Smith’s ECG Blog: 2015-10-06