- HPI: 80-something woman who presented with chest pain and dyspnea
- Course: acute MI was ruled out by serial troponins
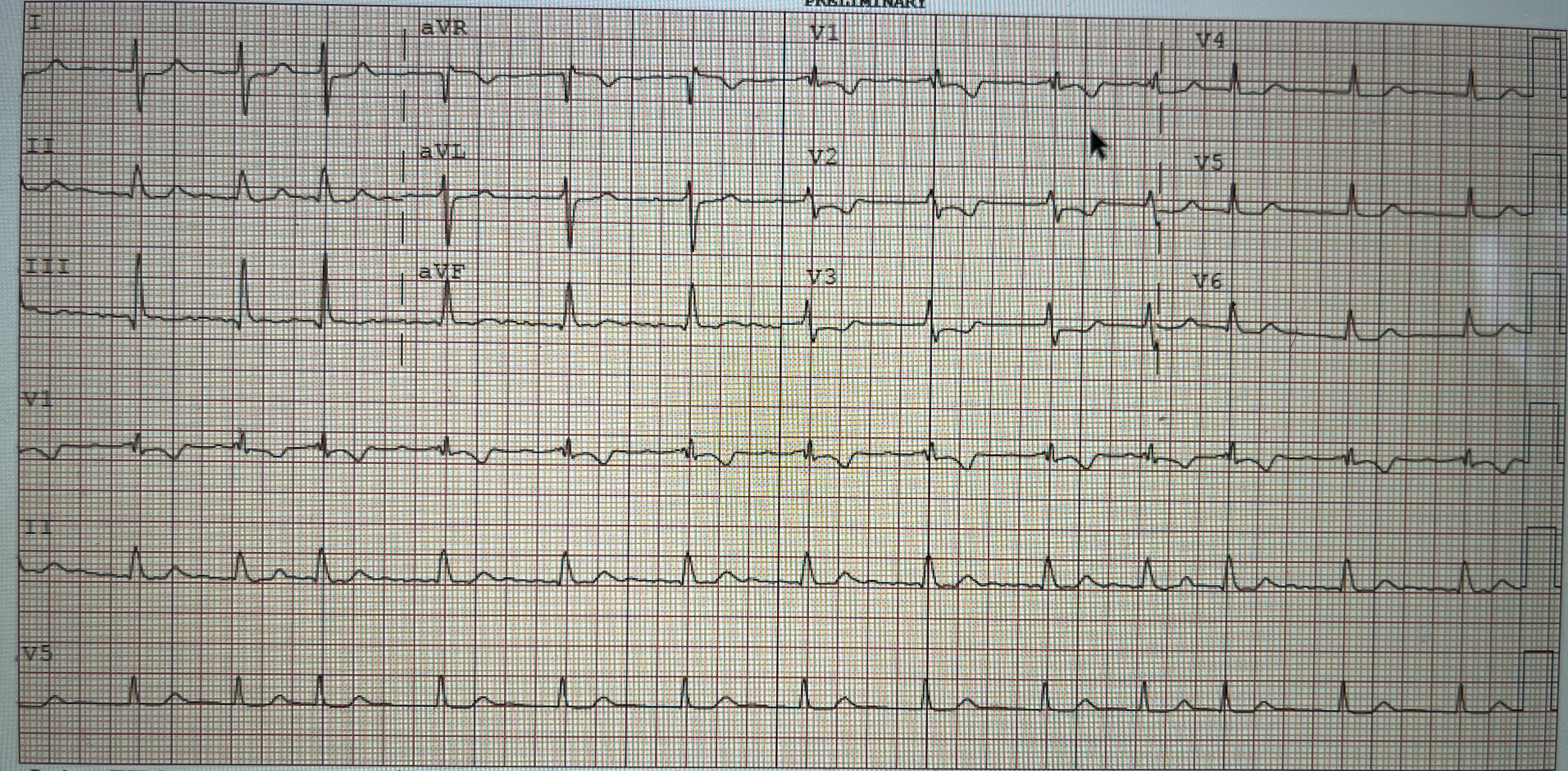
- ECG: There are small Q waves in leads III and aVF. These are probably not significant. Regarding R wave progression — the QRS complex in lead V1 is not “normal”. Instead — there is what appears to be an rsR’ configuration, with essentially no negative deflection following the R’. In adults — it is not normal for the R wave in right-sided lead V1 to be taller than the S wave is deep. This is because of left ventricular predominance in adults. As a result — the finding of a Tall R Wave in Lead V1 (ie, R=S or R>S in V1) should prompt the following diagnostic considerations: i) WPW; ii) RBBB; iii) RVH; iv) Posterior MI; v) HCM (Hypertrophic CardioMyopathy); and, vi) Normal Variant (which is a diagnosis of exclusion!). As per Dr. Smith — there also appears to be RVH in ECG #1 — because there is a predominant R wave in lead V1 + a rightward axis + incomplete RBBB + low voltage + ST-T wave abnormalities in anterior leads potentially consistent with RV “strain” — with this making 4 ECG findings potentially consistent with RVH in this patient who presented with acute dyspnea
- Link to full case @ Dr. Smith’s ECG Blog: 2023-07-7