- HPI: 70M with chest pain x 1 hr
- Cath: 100% thrombotic acute D1 occlusion, stented.
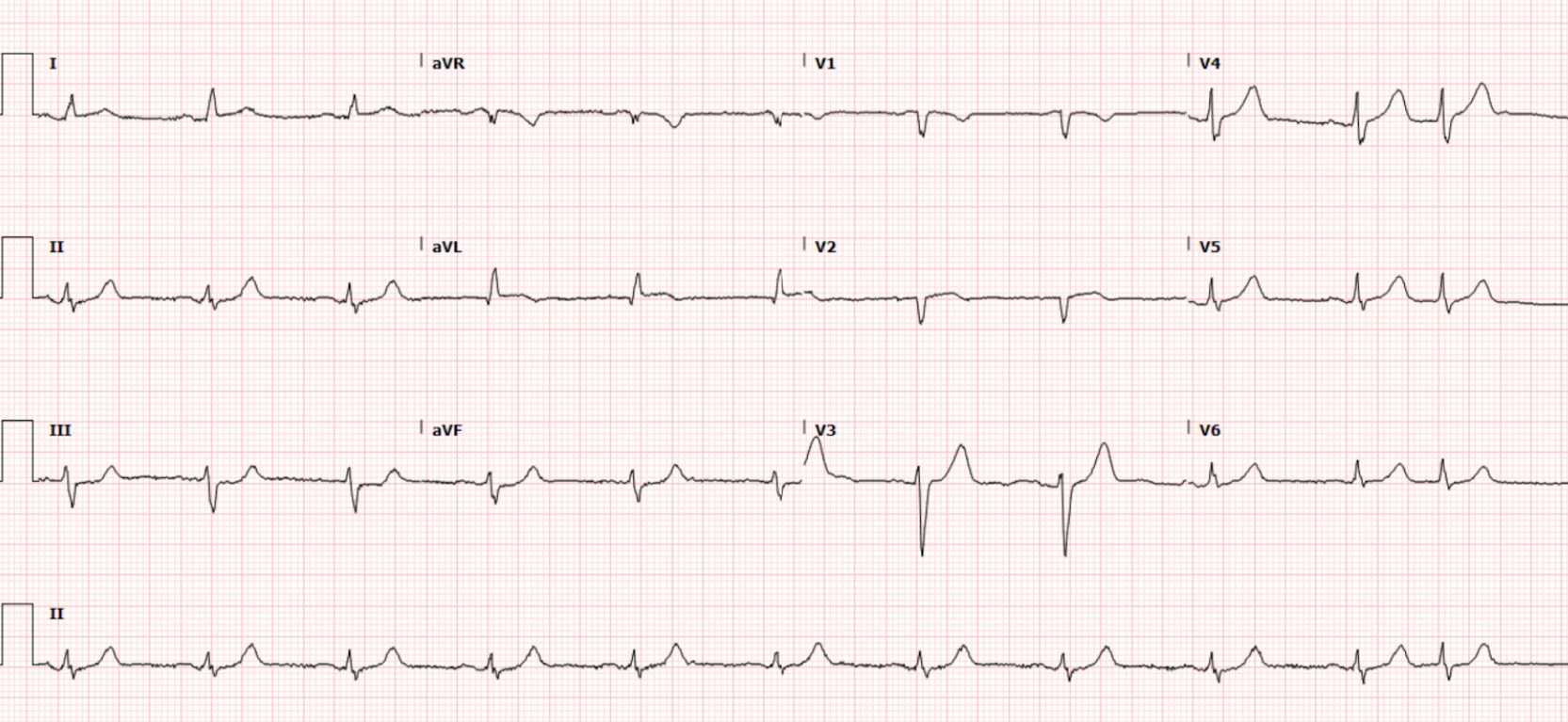
- Key ECG: The lead that caught my eye was lead aVL. The shape of the subtle-but-real ST elevation in this lead is not normal. Adding to my concern is the small q wave, and hint of beginning T wave inversion. This is not the appearance of a repolarization change. In view of the abnormal appearance in lead aVL — the subtle ST elevation in lead I (the dotted RED line in this lead) suggests a similar ongoing process in this other high-lateral lead. Confirmation that the lead aVL appearance is likely to be acute — is forthcoming from reciprocal changes in all 3 inferior leads (II,III,aVF). The ST segment straightening that we see in these leads (as per the RED lines) — that then leads up into clearly disproportionately tall T waves (considering the modest R wave amplitude) is not normal.
- Link to full case @ Dr. Smith’s ECG Blog: 2022-05-11
-USE.png){kind=link}