- HPI: 77F acute chest pain and SOB
- Cath: LCx large codominant, normal appearing until point of occlusion in mid-vessel
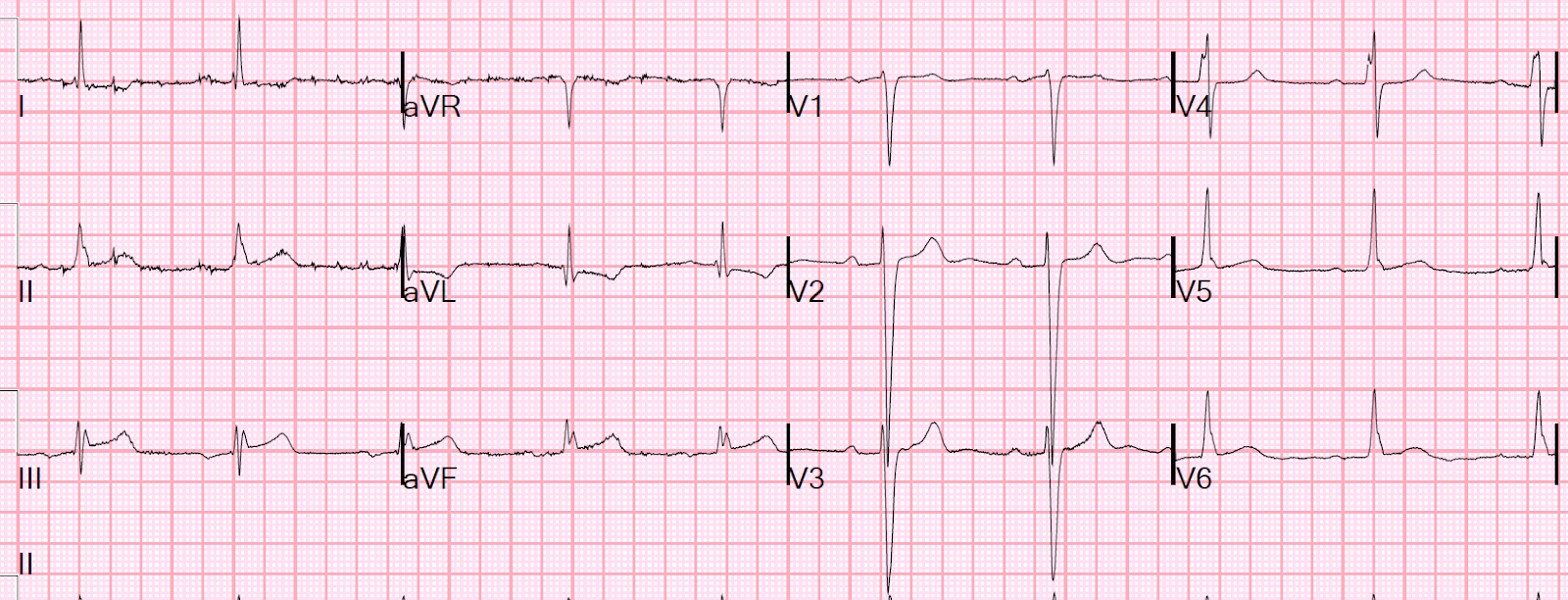
- Key ECG: There is ST elevation in inferior leads, with reciprocal ST depression in aVL, so one must strongly suspect acute inferior MI. However, 3 features should provide pause for poassible false positive (pseudoOMI): 1) There is LVH, 2) There is an intraventricular conduction defect, with QRS duration of 125 ms, 3) There is an RSR’ (saddleback) in lead III. This patient clearly has underlying structural heart disease (based on the intraventricular conduction delay) — and that can affect ST-T wave appearance appearance in a way that is hard to determine without seeing a baseline ECG
- Link to full case @ Dr. Smith’s ECG Blog: 2019-03-18