⚠️Note:
- Acute OMI with preservation of LVH voltage criteria is rare
- In most cases, acute LAD OMI causes diminution of S-wave voltage in V1-V3, which makes finding examples of OMI which preserve LVH voltage criteria unusual
🚨 Suggestive of OMI:
- Discordant STE > 1/6 (17%) preceding S-wave
- STE in V1-V3 > 25% of the preceding QRS
- This is very insensitive: STE in LVH rarely exceeds 4 mm. If an S-wave is 30 mm in depth, STE would have to exceed 7 mm to meet criteria.
- Symmetric TWI is more suggestive of ischemia (Figure from Dr. Ken Grauer )
✅ Expected ST changes in LVH:
- STE in leads with deep S waves (usually V1-V3) may mimic STEMI. This may be seen in LVH
- LVH usually has concave-upwards ST segments, but conVEX-upwards can also be seen
- LV “strain”:
- ST-T wave changes of LV “strain” in response to marked LVH are most commonly seen in one or more of the lateral leads (ie, leads I, aVL; V4,V5,V6).
- In its most extreme form — these changes manifest as asymmetric ST depression (ie, the ST segment descends slower than it rises)
- Instead of seeing ST-T wave changes of LV “strain” in lateral leads — some patients manifest a “mirror-image” of strain in anterior leads
- Use of the Mirror Test (ie, inverting the QRST complex in lead V1) may facilitate recognizing what the shape of LV “strain” may look like in a right-sided lead (such as lead V1 or V2). Example from Dr. Ken Grauer
- Some patients with LVH (especially if the frontal plane axis is vertical) — also manifest ST-T changes of LV “strain” in the inferior leads.
- The increase in leftward and posterior forces may overshadow baseline anterior forces — with a “net result” that R wave progression is delayed (sometimes to the point of producing QS complexes in one or more anterior leads).
- Inferior STE with reciprocal ST depression in aVL is frequently found in the following STEMI mimics: LVH, LBBB, inferior LV aneurysm, myocarditis
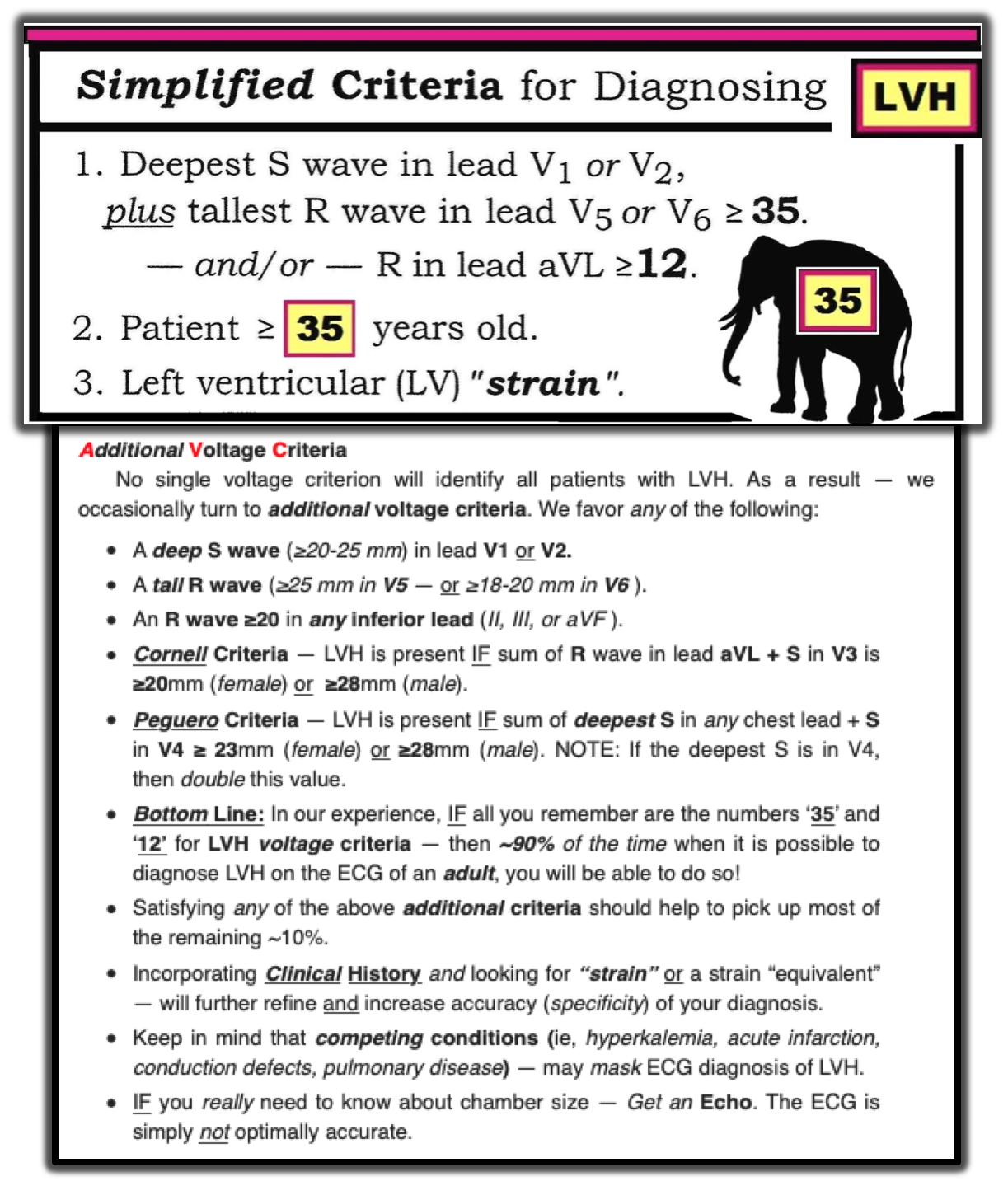
📝 LVH Criteria:
- Sokolow-Lyon
- [S wave V1 or V2] + [R wave V5 or V6] > 35 mm
- Sensitivity: 14%
- Specificity: 99%
- Modified Cornell
- [R wave aVL] > 11 mm
- Sensitivity: 14%
- Specificity: 92%
- Cornell
- [R wave in aVL] + [S wave in V3] > [28 mm for men] or [20 mm for women]
- Sensitivity: 31%
- Specificity: 93%
- Peguero
- [Deepest S wave in any precordial lead] + [S wave V4] > [28 mm for men ] or [23 mm women]; if deepest S wave is in V4, double this value
- Sensitivity: 57%
- Specificity: 90%
- Summary Figure from Dr. Ken Grauer
{kind=link}
{kind=link}
{kind=link}
{kind=link}