- HPI: 50M with chest pain x hours
- Cath: LAD D1 thrombus
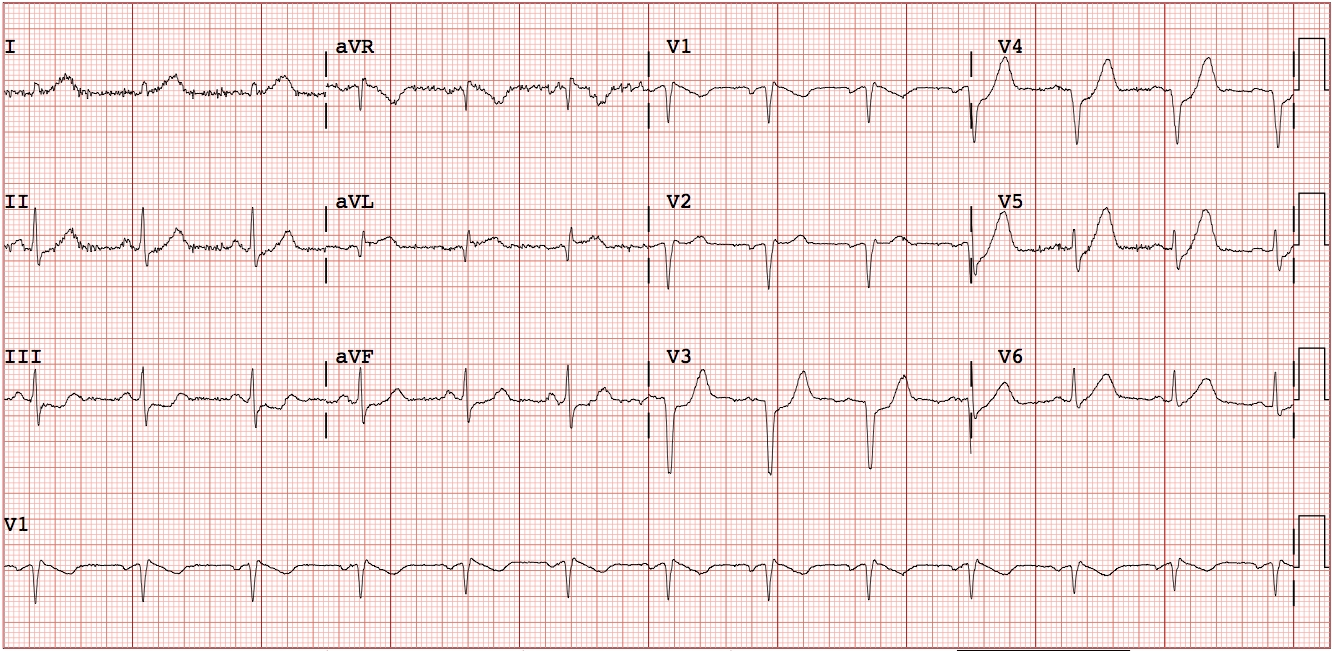
- Key ECG: There is approximately 1mm STE in aVL with reciprocal STD in II, III, and aVF. There is STD in V3-V6, with hyperacute T waves (de Winter’s morphology) in V3-V6 and also hyperacute T waves in leads V5, V6, and I. This is highly suggestive of acute transmural injury to the anterior and lateral walls, with the most likely etiology being acute occlusion (or near occlusion) of a coronary artery supplying these walls, such as the LAD, large diagonal, ramus intermedius, or sometimes the LCX or its branches. This morphology is distinctly de Winter’s T-waves. The de Winter pattern is characterized by ST depression and hyperacute (large) T-waves in the distribution of the ischemia. This is in contrast to upright T-waves from posterior MI, and also in contrast to the inferior ST depression in this case, which is reciprocal to the STE in aVL. In de Winter’s T-waves, if the ischemia worsens before reperfusion, the ST depression may evolve into ST elevation with or without hyperacute T-waves.
- Link to full case @ Dr. Smith’s ECG Blog: