- HPI: 50M with chest pain
- Cath: 100% proximal thrombotic occlusion of the LAD.
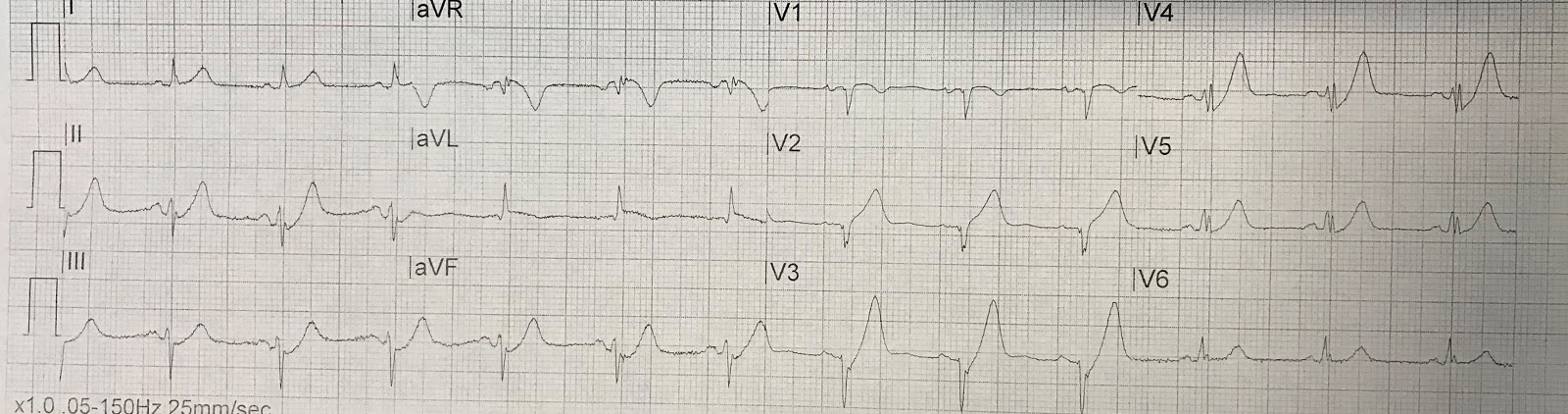
- Key ECG: There is sinus rhythm with perhaps 1mm STE in aVL, and also in V2 with hyperacute T-wave. There is STD in V3-V5, as well as II, III, and aVF, with hyperacute T-waves in all these leads as well, thus de Winter’s pattern in the anterior and inferior leads. This is essentially pathognomonic for Occlusion MI of the anterior and apical walls (de Winter pattern more likely represents ~99% thrombotic stenosis with just a trickle of flow, but essentially the same overall event, with progression to full occlusion extremely likely). The OMI is therefore occurring in the LAD, and the LAD is likely a type III “wraparound” which supplies the apical and distal inferior wall in addition to the anterior wall. Aside: This case proves that de Winter’s waves are not limited to anterior leads, but may be seen in any location. This is similar to Wellens’ waves, which were first described in the LAD distribution, but may occur in inferior and/or lateral leads as well.
- Link to full case @ Dr. Smith’s ECG Blog: