- HPI: Middle aged adult with acute chest pain
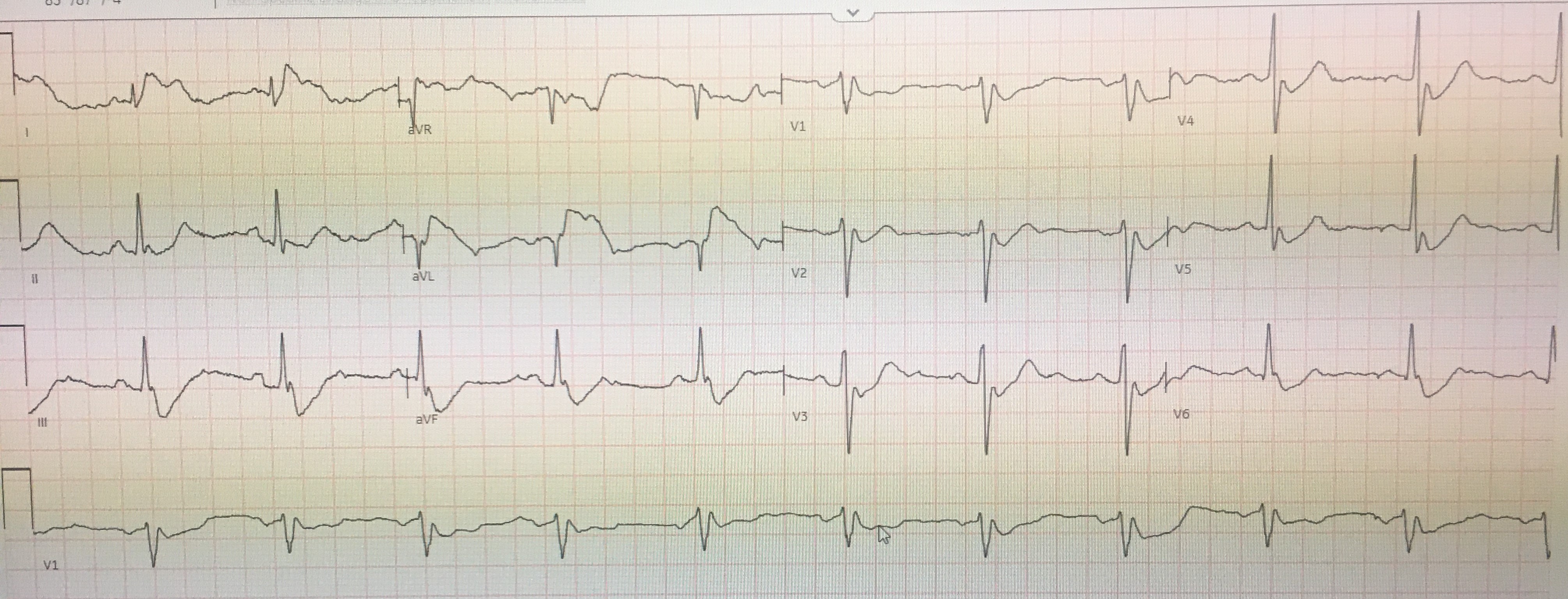
- Key ECG: The 1st thing to notice is that there is a tremendous amount of baseline artifact. This is especially true in the limb leads — where none of the seemingly elevated and depressed ST segments look the same. In the long lead V1 rhythm strip — each of the 10 beats manifest a different variation on the shape of the ST segment. When there is much artifact elsewhere on a tracing — the chances increase greatly that artifact is also affecting the ST segments you are concerned about. CLUE #2: The shape of the elevated and depressed ST segments in the limb leads is bizarre. The ST segment is jagged in the 2 limb leads with ST elevation (ie, leads I, aVL) — and the deepest part of the depressed ST segments in leads III and aVF is almost pointed. CLUE #3: The shape of the depressed ST segments in all 6 chest leads looks very similar (ie, with a “rounded scoop”, showing approximately the same amount of ST depression in each of these 6 leads — as highlighted in GREEN). The presence of geometric shapes (in this case, the “rounded scooping”) — is also unlikely to be physiologic. CLUE #4: All of the above described unusual shapes (ie, the peak of the ST elevation in leads I,aVL — the negative peaking in leads III and aVF — and the lowest part of the rounded GREEN scoopings) — occur at a fixed interval with respect to the preceding QRS complex. This suggests us that whatever is producing these deflections must be related to cardiac contraction (and/or to arterial pulsation)! CLUE #5: The distribution in ECG #1 of the bizarre ST-T wave deflections precisely follows the location and relative amount of amplitude distortion predicted by Einthoven’s Triangle.
- Link to full case @ Dr. Smith’s ECG Blog: 2022-08-26