- HPI: 40M with HTN presented with acute onset chest pain, diaphoresis and SOB
- Cath: Thrombotically or embolically occluded RCA at bifurcation to the RPDA and RPLA.
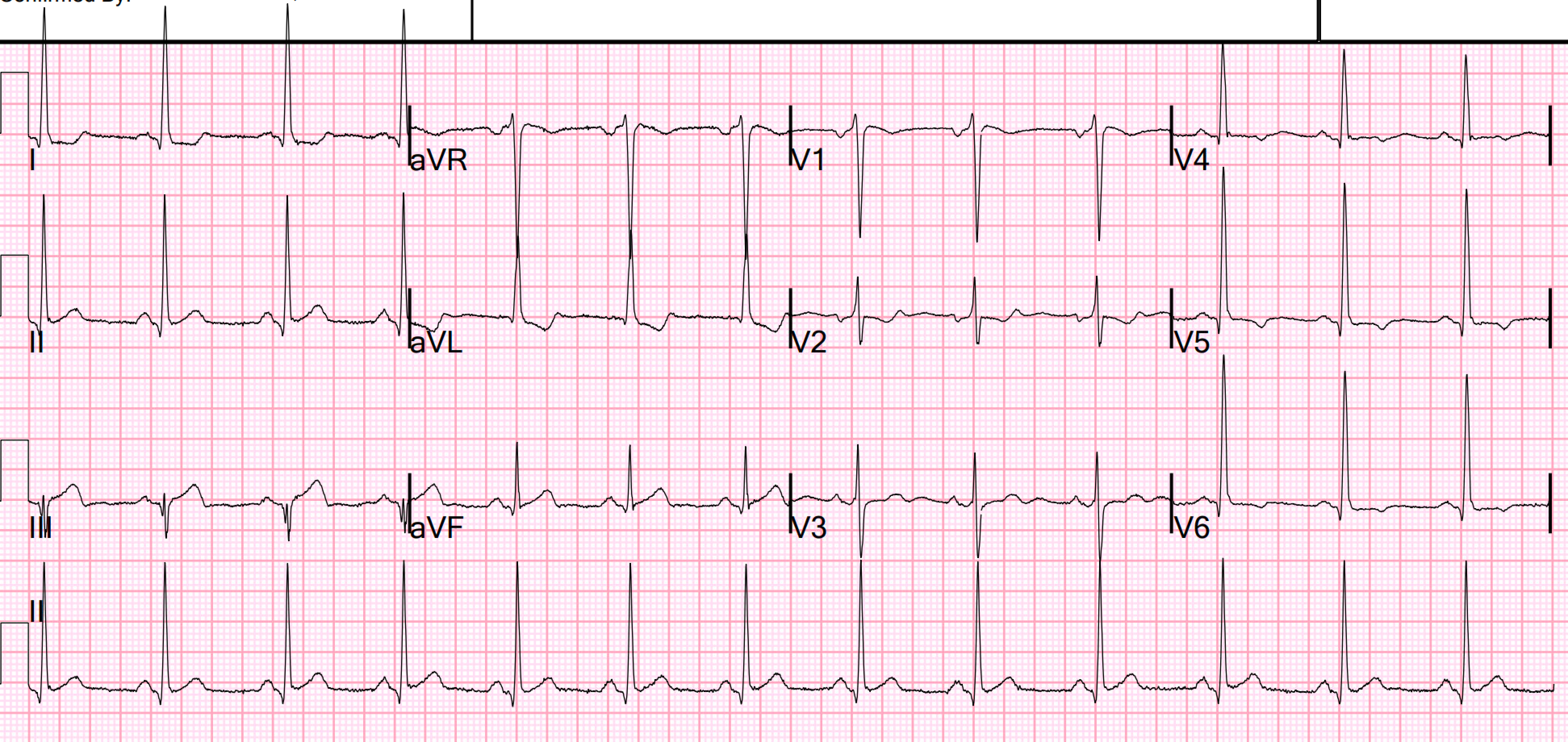
- Key ECG: It is tricky because it is in the setting of LVH. See V2: there is downsloping ST segment. The T wave in lead III Is too big for that small S wave. There is terminal QRS distortion in aVF. The STT in aVF is not discordant as you would expect with LVH, and there is a straight ST segment. The abnormal shape of the ST-T wave in lead V2 also constitutes a positive Mirror Test. Even without LVH — the taller-than-expected initial R wave in lead V2 and the ST-T wave appearance in this lead instantly suggested to me that posterior OMI was likely
- Link to full case @ Dr. Smith’s ECG Blog: 2022-09-30